
BERLIN – Refractive laser surgery is currently performed without monitoring the ongoing ablation process. An optical system using an ultraviolet fringe projector has been developed for online monitoring of the amount of tissue ablated during excimer laser procedures for refractive corrections. The system is an add-on device which uses the ultraviolet wavelength of the laser pulses for continuous intraoperative topometry. Excimer laser refractive corneal surgery has found widespread acceptance throughout the world. About 500,000 patients were treated in the US in 1998, and a further increase is expected owing to the permission recently granted by the Food and Drug Administration (FDA) for two additional companies to enter the US market. Several other companies will also have passed their FDA trials for such laser systems in the near future. Refractive laser procedures are commonly performed according to nomograms based on empirically collected data . Nomograms are guidelines enabling the selection of appropriate laser parameters for each individual correction. They take into account factors found to influence the refractive outcome by the physician or manufacturer who established them. It is reasonable for refractive laser procedures to aim at slight myopia rather than planocorrection because the biological tissue variance (e.g., humidity ) prevents standardization, so that the exact outcome cannot be guaranteed. Physicians therefore prefer to undercorrect, since the eyes would have much more difficulty compensating for overcorrection, particularly those of the elderly. Another issue of major current interest is topography-based laser correction. These corrections adjust laser parameters to topographic maps previously acquired to make allowances for asymmetric surface alterations. However, the time delay between the topographic exam and the laser treatment might cause lateral adjustment errors of the eye and consecutive eccentric or false axis corrections. Moreover, the accuracy of currently available topography devices in providing elevation maps is debatable. Several companies are currently aiming at customized corneal shaping based on wavefront aberration measurements. Since these measurements cannot be done online either, however, the problems involved are similar to those encountered with topography-guided treatment. To overcome the aforementioned problems, we have developed a system for online monitoring of the amount of tissue removed by the laser. The main principle of operation has been adopted from an interferometric technique called fringe projection. In conventional interferometry, fringes are produced using coherent light sources that interfere with one another in different ray paths to provide height or structural information on the surface of an object. If lower resolutions suffice, fringes might also be projected using appropriate imaging optics.
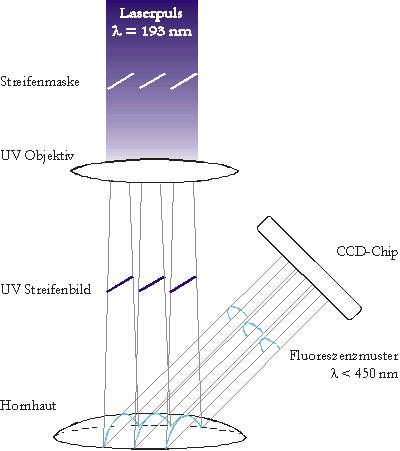
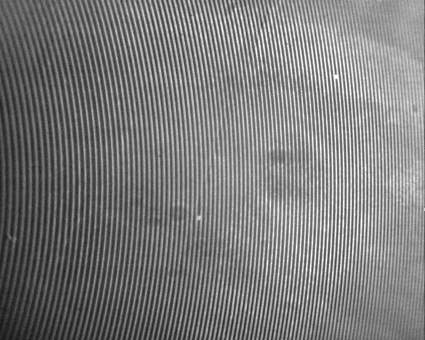
Figure 1 shows the principle of operation. The ultraviolet laser pulse is guided through a partly transparent grating (e.g., a Ronchi Ruling). This grating is imaged onto the cornea using an optical system of quartz lenses. It has been shown that the UV light emitted by the ArF excimer laser only penetrates the corneal tissue for the fraction of a micrometer. This makes the laser suitable for precise reshaping of the corneal surface. The projected UV light pattern excites the corneal tissue to emit fluorescence. The shallow penetration depth guarantees that the fluorescence signal only comes from the outermost layer. The fluorescence was found to have a wavelength ranging up to 450 nm. Conventional CCD cameras are already sensitive in this spectral range. Since structured UV radiation is used, a corresponding pattern of fluorescence is detected. The camera is obliquely oriented to the direction of projection and thus views the fluorescence pattern as deformed compared to the one originally projected. The image on the left side of Figure 2 gives an example of a fluorescence pattern on a porcine cornea as viewed with a digital camera (Hamamatsu Orca). The deformation of the pattern is directly related to the elevation map of the cornea. Established algorithms are used to compute these elevation maps from the fluorescence patterns .
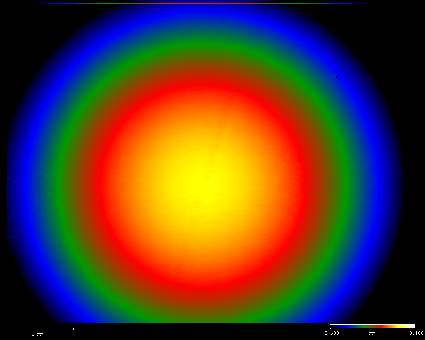
The picture below of Figure 2 shows an elevation map that corresponds to the fringes on the left.
Calibration and testing of the device is achieved using optical surfaces of high-quality lenses for visible light. These lens surfaces are known to be manufactured in a quality exceeding lambda/2 with lambda in the visible range of the spectrum. Under 193 nm irradiation, the lens material (BK7) exhibits characteristics similar to those of corneal tissue with respect to the penetration depth and fluorescence emission. The left side of Figure 3 shows the fringe image of a planoconvex lens with a focal length of 40 mm (Spindler & Hoyer) and a surface radius of ...mm. Analysis of the image yielded the elevation map on the right with a radius of ... The energy density of the laser pulses emitted for the topometry is in an order of magnitude below the ablation threshold. The fluorescence is excited by only 5 mJ/cm_ on a circular area 10 mm in diameter. Since the ablation threshold for the ArF excimer laser is about 20 mJ/cm, tissue alterations are clearly excluded . Typical treatment energy densities range from 100 mJ/cm to 250 m/cm, which is more than an order of magnitude higher than the value for fluorescence excitation. The grating has equal spacings and line widths of 100 microns. The camera has a lateral resolution of 10 microns per pixel. The height resolution is approximately 2 microns. The boundary conditions for incorporating the system into a medical laser vary with the manufacturer and the model. Large-area laser pulses either have to be attenuated or partly reflected using a beam splitter. Flying spot lasers can be operated in such a way that the laser pulse is reflected into the measuring system by the scanner. It seems feasible to connect the topometry system to the eye-tracking device of the laser. A new device has been proposed for online monitoring of the ablation process during laser refractive surgery. We expect this device to eliminate the need for nomograms and conventional-topography-based corrections. Treatment planning should therefore include wavefront-aberration-based measurements converted to an elevation map using the described online measuring device. This will optimize both planning and treatment. |
Press Release dated 03.06.99 in English